30 y/o F with b/l pedal edema, SOB and b/l knee joint pain
35y/o woman with b/l pedal edema, SOB and b/l knee joint pain
Manvi Sharma
Roll no 88
2018 batch
16th March 2022
"THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE - IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS / HER /GUARDIAN'S SIGNED INFORMED CONSENT .HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS WITH AN AIM TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUT."
Chief complaints -
A 35 y/o female who is a housewife presented to the OPD with chief complaints of
high grade fever and cough with sputum since 5 to 6 days,
b/l pedal edema (pitting type) since 5 days
and difficulty in breathing even at rest or after talking (grade 4) since 5 days

History of presenting illness -
The patient was apparently asymptomatic 1 yr back when she developed b/l knee joint pain and itching in upper aspect of chest and neck.The pain was insidious in onset and gradually progressive and also associated with morning stiffness. She was taking medication for this(?)
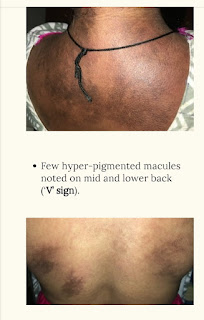
At the same time she had itching over neck and chest due to which the area turned red and then black.
She also complained of generalized pain and muscle weakness of the proximal and distal(?) muscles since 1 yr
There was complaint of b/l pedal edema and sob(grade 3) since 6 to 7 months which was gradually progressing to the present state.
C/o vaginal discharge 8 to 9 months back which was curdy white amd later changes to watery.
C/o oral and genital ulcers since 1 yr
C/o loss of taste since 8 months
C/o throat pain since 8 months
C/o weight loss over the last 1 yr (?)
About 2 months back she came to the hospital with the above mentioned complaints and was diagnosed with DERMATOMYOSISTIS with vaginal candidiasis and given the following treatment -
1.tab.wysolone 50mg po od
2.syp.mucaine 10ml/po/tid
3.tab.ultracet 1/2 po/QIT
4.candid cream for L/A
Patient was referred to other health centre for muscle biopsy.
Her ANA immunofluoroscence showed homogeneous pattern.Intensity 4+ associated antigens involved-ds DNA,histones.
HRCT was done -
IMPRESSION: Few patchy areas of ground glass opacities in peri bronchovascular distribution-s/o pneumonitis (Corads-4)
Her images from 2 months back -



Treatment given -
1.TAB.CALTEN
2.TAB.AUGMENTIN
3.TAB.NAPROXEN SODIUM
4.TAB.FOLVITE
5.CANDID CREAM
6.TAB.WYSOLONE
7.TAB.ESOMEPRAZOLE
8.TAB.SODIUM ALENDRONATE WEEKLY ONCE.
Previous X-RAYS -











Comments
Post a Comment