Note - This is an a online e log book to discuss our patient's de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centred online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment.
DOA - 20/11/23
Case -
A 77 yr old man was brought to the GM OPD with chief complaints of
• vomitings since yesterday night
• loose stools since yesterday night
• generalised weakness since yesterday
History of presenting illness -
Patient was apparently alright till yesterday night. He gives history of consuming food outside at a function following which he developed vomitings about 4 episodes, which is black in colour, projectile, watery, non bilious with no food particles. Vomitings are associated with loose stools about greater than 5 episodes, mucoid in consistency, black to dark brown in colour, non-blood stained, no bleeding per rectum. Symptomatic treatment was given at home following which next day they came to our hospital with c/o excessive whole body weakness.
No h/o pain abdomen, fever, cough, cold, breathlessness, burning micturition, chest pain, palpitations, excessive sweating, paraoxysmal nocturnal dyspnea, bleeding manifestations
H/o hiccups +
H/o urinary incontinence +
Past history -
Patient is not a k/c/o DM, HTN, TB, asthma, epilepsy, CVA, thyroid disorders
K/c/o CAD 2 yrs back, s/p - PTCA (left anterior descending artery)
Treatment history -
Some of the medications he is using outside
Personal history -
Appetite - normal
Diet - mixed
Bowel - regular
Micturition - normal, incontinence +
No known allergies
No addictions
Family history -
No significant family history
General physical examination -
Pt is conscious, coherent and cooperative and well oriented to time, place and person.
Pallor +
No icterus, cyanosis, clubbing, lymphadenopathy and edema
Vitals on admission -
Temp - 98.6F
BP - 130/60 mm hg
PR - 94bpm
RR- 18cpm
Grbs - 138mg/dl
SpO2 - 94% @ RA
Systemic examination -
CVS - S1, S2 heard, no murmurs
RESP SYS - trachea - central , bilateral air entry +, NVBS heard, crepts heard in RT infra -axillary region
PER ABDOMEN - soft, non tender, no organomegaly, bowel sounds heard
CNS - NFND
Provisional diagnosis-
Acute gastroenteritis
CAD S/p PTCA (LAD artery)
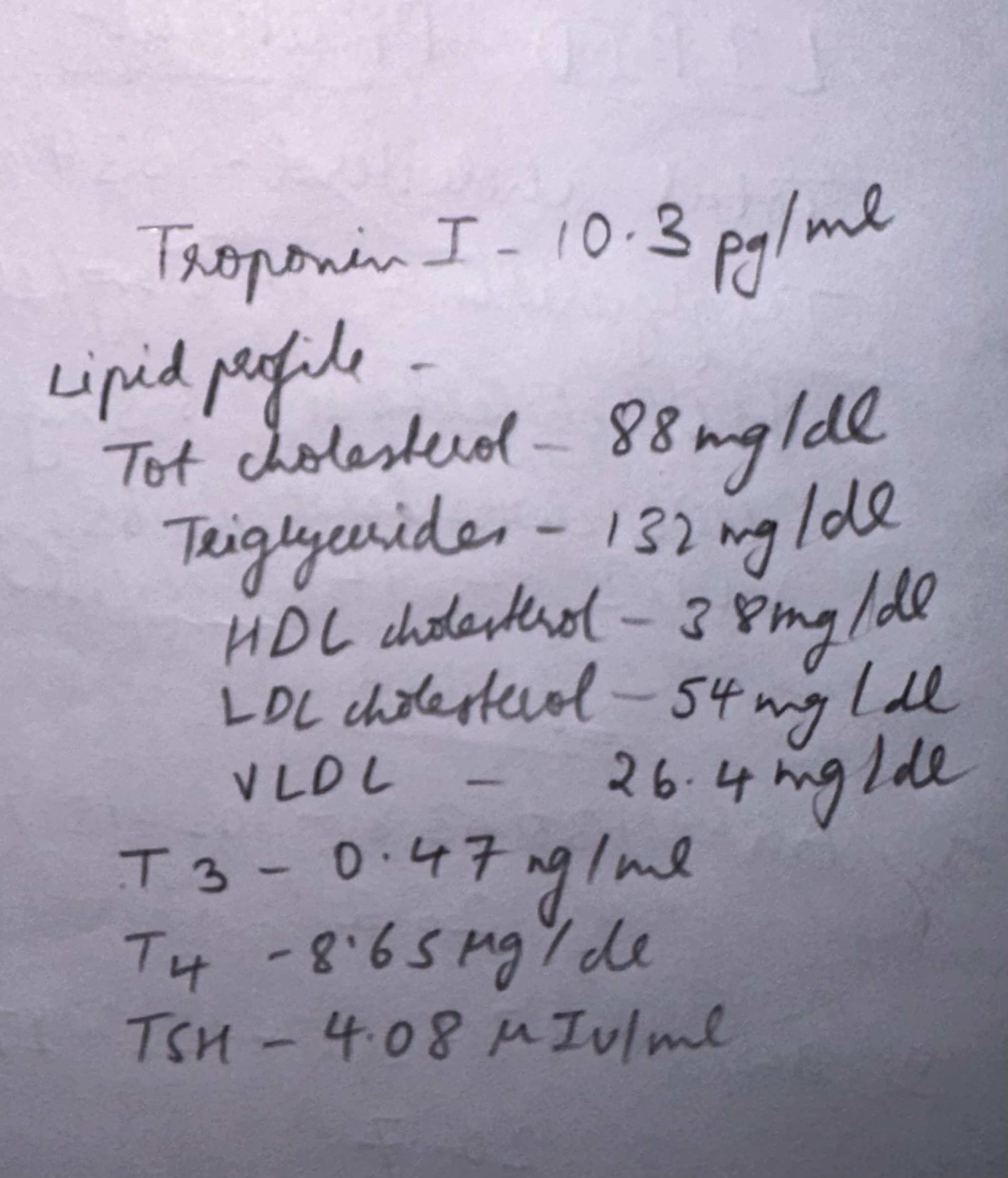
Investigations -
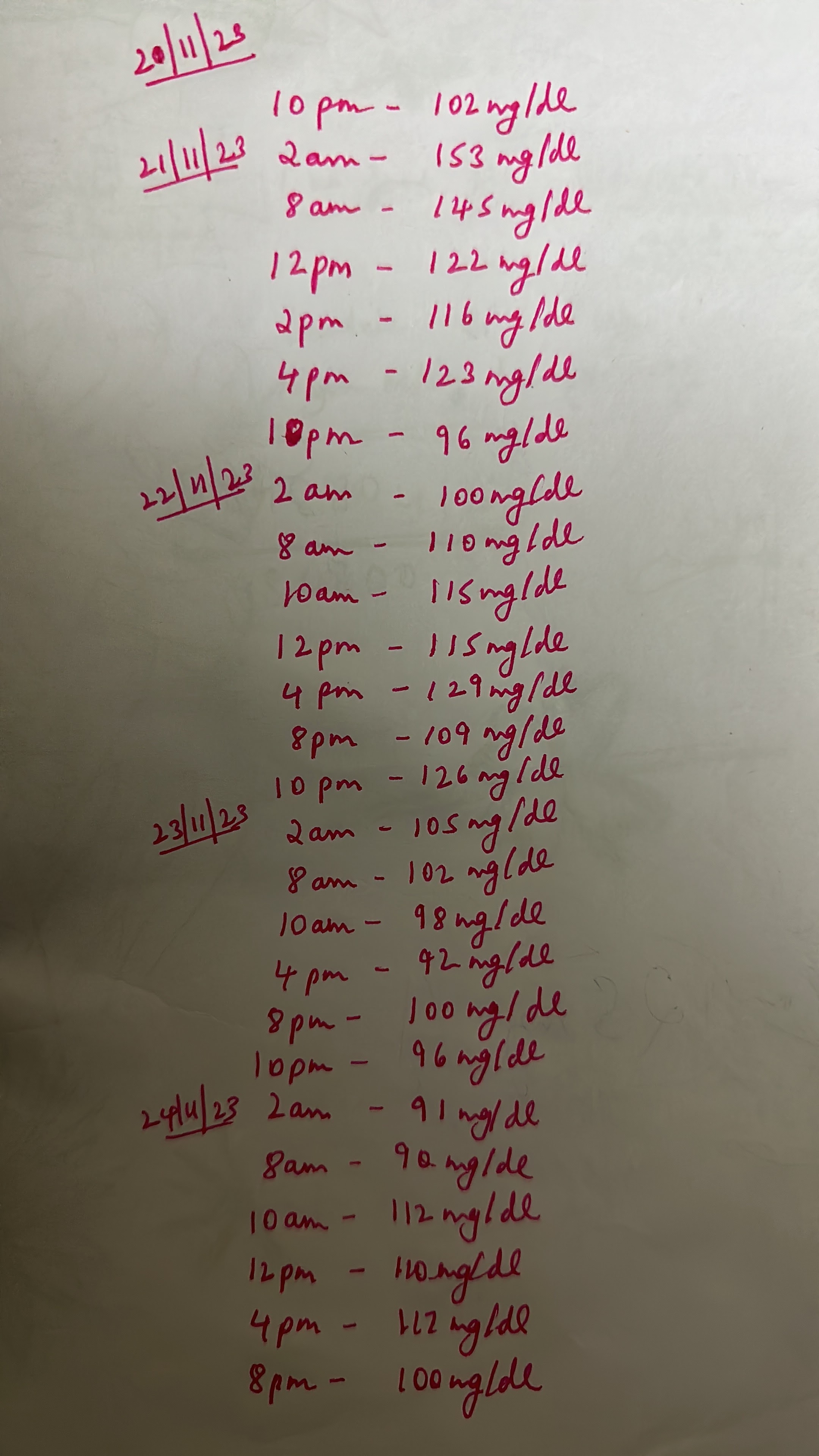
GRBS pre and post meal values -
Final diagnosis -
Severe anemia - iron deficiency anemia
Heart failure with preserved ejection fraction (EF-57%)
K/c/o CAD , S/p - PTCA 2 yrs ago (LAD artery)
Acute gastroenteritis (resolved)
Plan of treatment -
INJ CEFTRIAXONE 1gm IV BD
INJ PAN 40 mg IV TID
INJ EMSET 8mg IV TID
IV fluid NS & RL @ 100ml/hr
Tab TAXIM 200mg PO BD (8am——8pm)
Tab ROSUVASTATIN 20mg HS (9pm)
Tab ECOSPRIN 75 mg OD (8am)
Tab CLOPIDOGREL 75 mg OD (2pm)
Tab PROLOMET 25mg PO OD (8am)
Tab BISACODYL 5mg PO HS
INJ Iron sucrose 200mg in 100ml NS IV OD
Syrup GUT CLEAR 30 ml OD HS
Procto clysis enema stat
Tab Livogen PO OD
Strict I/o charting
3 units PRBC transfusion done
Upper GI endoscopy done
Upper GI endoscopy
Impression - large sliding hiatus hernia
multiple esophageal distal ulcers
multiple erosions in fundus
no blood seen in duodenum
GERD - severe erossive fundal gastritis
OSCE
What is hematemesis? Causes of hematemesis.
It is defined as blood in vomitus. It is due to bleeding that takes place in mainly upper GI tract above ligament of Trietz.
Various causes are -
• Most commonly - peptic ulcer (gastric or duodenal)
• Erosive gastritis
• Stress ulcers
• Esophageal varices
•Mallory-Weiss syndrome
•Carcinoma stomach
• Angiodysplasia or vascular malformations
Work up of hematemesis in this case.
Colour of the vomitus described as coffee brown
Also history of melena +
Blood urea (88mg/dl) increased significantly higher than serum creatinine (1.4mg/dl). This happens due to increased intestinal absorption of urea after breakdown of blood proteins. An elevated blood urea level with normal creatinine concentration implies severe bleeding.
Upper GI endoscopy done which revealed -
large sliding hiatus hernia, multiple oesophageal distal ulcers, multiple erosions in fundus
What is the cause of generalised weakness in this case?
It is probably due to the severe anemia that he is suffering from with a hemoglobin value of 3.9mg/dl at the time of admission.
Document the serial wise increase in hemoglobin values along with the intervention done.
Complications of blood transfusion. Acute -
Acute haemolytic reaction
Allergic reaction
Febrile reaction
Septic or bacterial contamination
Transfusion associated circulatory overload
Transfusion related acute lung injury
Delayed -
Delayed haemolytic reaction
Iron overload
Work up of anemia in this case.
The following investigations were carried out to find out the cause of anemia -
Peripheral smear - microcytic hypochromic RBCs
Serum iron - 52 micrograms/dl
Serum ferritin - 8.4ng/ml
Serum LDH - 177 IU/L
Stool for occult blood - negative
Serum vit B12 and B6 levels also adviced
Upper GI endoscopy to rule out upper GI bleed
What is the type of heart failure in this case and it’s mechanism?
The patient is suffering from heart failure with preserved ejection fraction (EF-57%)
Mechanism -
Enumerate the drugs used for heart failure.
Diuretics
ACE inhibitors
ARBs
Beta blockers
Aldosterone receptor agonists
Digoxin
Vasodilators - hydralazine and nitrates
Role and efficacy of anti-platelet therapy in CAD patients post CABG.
Reduces the risk of MI
Improves vein graft patency
Reduces the incidence of vein occlusion
Prevents thrombus formation and plaque rupture
In the large CURE trial, dual antiplatelet treatment with aspirin and clopidogrel led to a relative risk reduction of 20% for the combined end point of cardiovascular death, myocardial infarction and stroke compared to aspirin alone: 11.4% to 9.3%.
Even though this patient is non-hypertensive and non-diabetic, what is the precipitating factor for CAD and heart failure?
In this study, 120 non-diabetic cases were evaluated and 53.5% were males. Although an association was found between CAD and IR, more detailed analysis had notable findings. For example, the association between CAD and IR was found in non-diabetic men. This finding was not statistically significant in women. The average age of the population was 57.8±12.69 years and 60% of them were 50-70 years old. This is similar to Karrowni et al.'s study that showed the higher prevalence of CAD in the elderly and most of the patients were in the same age group. Although age is an important factor in CAD and IR, Kim et al. showed that age increase plays a role in elevating insulin resistance.In Schmiegelow et al.'s study, insulin resistance measures did not improve CVD risk discrimination and reclassification in postmenopausal women.In our study, CAD was more prevalent in patients over 70 years, while most IR was seen between 50-70 years. The reason for this finding is that people prone to type II diabetes whose disease have not appeared yet are in this group and the majority of people older than 70 years and with insulin resistance have been excluded from the study.






















Comments
Post a Comment